Oddly enough, the risk of developing depression during pregnancy is lower than at any other time in a woman’s life. However, depressive disorders and related conditions still occur. Moreover, at different times. On the other hand, all anxiety states typical of pregnant women cannot be attributed to depression. Fears for the life and health of the child, your own and his future, and financial resources are normal. The main thing is to make sure that these concerns remain within reason.
Symptoms of depression in pregnant women are almost the same as in other stages of life. Those. persistent decline in mood, decreased intellectual function, sleep problems, irritability, etc.
Depressive disorders often occur during pregnancy and pose a risk to the woman's health and the health and development of her child. Depression interferes with the ability to enjoy life, eat, sleep, work; blood pressure may rise, there may be insufficient weight gain, and there are mood swings from tearfulness, touchiness to aggression. Although generally anxious moods are typical for a woman during pregnancy, at this time she is especially susceptible and may experience fear of childbirth, especially if it is the first, and fears for her health and the health of the child. However, you need to understand that no matter how justified these fears are, they must still be within certain boundaries, otherwise we can talk about depression. A pregnant woman needs to cope with the disease as quickly as possible, preferably in the early stages. Psychotherapy plays a major role here; it is a very effective method of treating depression during pregnancy.
Psychotherapy is a system of medical psychological influences on the psyche that changes behavior, beliefs, and thoughts. A psychotherapist will help a woman tune in to positive thoughts, find peace of mind, correct distorted beliefs, and eliminate the causative factor. Psychotherapy can be individual or group. Experience shows that group psychotherapy is more effective in treating depression during pregnancy. Group members support each other and share their successes in overcoming the disease.
What are the dangers of depression during pregnancy?
Depression is a psycho-emotional disorder characterized by apathy, constant low mood, inability to rejoice and changes in thinking. A depressed person begins to think only about bad things, without perceiving anything good. A pregnant woman, on the contrary, needs to receive as many kind, joyful emotions as possible. But this is not the only danger of depression during pregnancy. As a result of this mental disorder, a person may begin to have thoughts of suicide. Instability of the emotional background can lead to addiction to alcohol and psychotropic substances. All this negatively affects the health of both the child and his mother.
Taking antidepressants - pharmacotherapy during pregnancy
Mild depression can be treated with psychotherapy, but if symptoms are moderate or severe (for example, suicidal thoughts), pharmacology is also necessary.
Antidepressants used during pregnancy are selective serotonin reuptake inhibitors (SSRIs) or serotonin norepinephrine reuptake inhibitors (SSRIs). Such medications should absolutely not be taken without the permission of a gynecologist!
Symptoms of depression
If you notice a couple of symptoms, you shouldn’t panic right away. You can assume the presence of a depressive disorder if five or more symptoms persist in you or your loved one for quite a long time, from two weeks or more. Signs of depression in pregnant women can be observed as follows:
- the woman feels depressed, her sadness is unfounded, she is apathetic
- you notice a person’s weakness, lethargy
- irritation
- negative vision of the future, feelings of hopelessness, tearfulness
- feeling of guilt, constant lack of self-confidence and the correctness of one’s choice
- feeling of helplessness and worthlessness
- Digestive problems: loss or increase in appetite
- insomnia, drowsiness, nightmares, sleep inversion
- various fears
- indifference to one's health
- reluctance to communicate with relatives and friends, with her husband.
Antidepressants and the risk of developmental defects
Treatment of depression with electroconvulsive shocks is not yet particularly popular. Psychotherapy is most often recommended for pregnant patients and, in some cases, antidepressants are prescribed. And here the question arises: can these drugs have a negative effect on the child?
Studies on the harmful effects of antidepressants on the fetus bring conflicting results - some indicate an increased risk of various types of defects in the child, others do not confirm such relationships. This explains why patients suffering from depression are most often advised to stop taking antidepressants before becoming pregnant, and if they become ill only during pregnancy, to try psychotherapy.
In situations where untreated depression poses a great danger to the mother and therefore to the child, medication is of course necessary. Currently, SSRIs (selective serotonin reuptake inhibitors) and SSRIs (selective serotonin and norepinephrine reuptake inhibitors) are considered the safest for the developing fetus and the woman herself. However, these are the most commonly prescribed drugs - except for paroxetine, which significantly increases the risk of heart defects in children.
Depression during pregnancy is much less commonly treated with tricyclic antidepressants, although most studies show no link between this type of drug and the risk of malformations (defects) in the fetus.
What are the characteristics of depression during different periods of pregnancy?
A pregnant woman does not immediately get used to the idea that she is now a mother and that her life will change a lot. In the early stages of pregnancy, she may forget about her situation, to the point that, for example, she makes grandiose plans for the near future, without taking the child into account. Depression during pregnancy at this stage can occur due to the woman’s unwillingness to part with her favorite job, growing career, study, or usual way of life. It also happens that a woman has been waiting for a child for a long time, she previously had miscarriages, a frozen pregnancy, or she simply could not get pregnant, and now, when this finally happened, she begins to be overcome by fears. She fears for the baby's health because she doubts her ability to give birth to a healthy baby. In this case, if it has not reached the point of depression, you can simply get yourself and your child examined to calm down.
In the second trimester, depression in pregnant women appears for other reasons. The woman is already aware of her position, moreover, it in itself becomes more noticeable both to her and to those around her. Experiences associated with this and with the child’s future can give rise to depression.
In the later stages of pregnancy, a woman becomes increasingly frightened by the inevitably approaching birth. At the same time, a pregnant woman may worry not only about herself, but also about ensuring that the baby is not harmed during childbirth. They begin to be overwhelmed by thoughts about how difficult it will be with a child, fears that the woman herself will not be able to raise a child.
Depression undoubtedly has a negative impact on the health of mother and child.
Psychotherapy during pregnancy
Currently, the most recommended form of treatment for mood disorders is cognitive behavioral therapy. During subsequent sessions, the expectant mother learns to correctly interpret various life situations and respond to them appropriately, due to which her level of anxiety decreases.
Cognitive behavioral therapy focuses on the “here and now”—during meetings with a psychotherapist, a person does not dwell on events from the past. You should also know that this is short-term therapy - most often it ends after about twenty consultations.
Baby blues and postpartum depression
Pregnancy and childbirth are stressful events for the somatic and mental state of a woman. The most common mental disorders of the postpartum period include postpartum depression and a symptom complex referred to as “baby blues” or “maternal blues”.
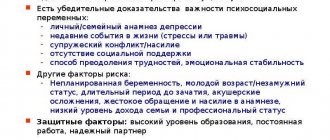
Data from various studies indicate that postpartum depression in the first months after childbirth occurs in 10–20% of women. Factors that increase the likelihood of developing this disease are: the presence of anxiety and depressive conditions in the prenatal period, episodes of depression, mental trauma during pregnancy, emergency caesarean section and complications during childbirth, illness of the newborn, lack of support from the immediate environment. Postpartum depression is characterized by feelings of depression, despondency, weakness, and high levels of anxiety. This disorder is also characterized by decreased appetite, sleep disturbances, a pessimistic assessment of life prospects, slowed thought processes, apathy, and lack of motivation for any active action.
Many studies indicate that the main role in the development of postpartum depression belongs to hormonal changes that occur in a woman’s body. The steroid hormones progesterone and estrogen are important for the normal course of pregnancy and the processes of changes in the body. The concentration of these hormones is characterized by a slow increase during pregnancy, and in the later stages it is several hundred times higher than the normal level. After the birth of a child, the level of hormones drops sharply, which becomes a great stress for the woman’s body and affects her mental state.
Progesterone, which acts on neurons through a classical genomic mechanism, also has the potential for rapid membrane action. The genomic mechanism involves influencing intracellular receptors at the nuclear level: stimulation of these receptors leads to changes in the synthesis of enzymes and neurotransmitters. The rapid membrane action, in turn, is responsible for the anesthetic effect of progesterone. Women who experience a sharp drop and lower progesterone levels in the postpartum period compared to average levels are more likely to suffer from depression. A similar situation is observed when the amount of estrogen in the blood plasma changes. Some studies indicate that taking hormonal medications to increase estrogen levels has been shown to be effective in treating postpartum depression. There is evidence demonstrating a connection between the occurrence of thyroiditis in the puerperia (postpartum period - editor's note), leading to disruption of the thyroid gland, and episodes of postpartum depression. However, this connection was found only in women with elevated levels of antibodies to thyroid cells.
In addition to hormonal changes in a woman’s body, a number of authors assign a significant role in the development of postpartum depression to psychogenic factors. Thus, an obstacle to satisfying social needs after the birth of a child, while their personal significance is high, creates a situation of frustration, which is a source of constant stress. Social and psychological factors such as the level of marital satisfaction and social support of a woman, according to a number of studies, correlate with the severity of postpartum depression, while these factors are less associated with the frequency of diagnosis. Depressive disorder is characterized by increased fatigue, decreased physical activity, and apathy, but women in the postpartum period are often forced to care for the child even in this state, which, firstly, becomes an obstacle to diagnosing depression, and secondly, can aggravate its symptoms.
Postpartum depression is a fairly well-studied mental disorder, which cannot be said about the so-called “maternal blues” or the sadness syndrome of women in labor - a symptom complex that, according to various researchers, occurs in women in Puerperia with a frequency of 15 to 80%.
Baby blues are characterized by mood lability, sharp reactions to minor events, tearfulness, and absent-mindedness. Typically, this condition manifests itself in the first time after the birth of a child, reaches a peak on days 5–6 and gradually subsides. Due to the fact that maternity sadness syndrome is highly prevalent and usually resolves quickly, this condition is not considered a serious problem in clinical practice. However, there is evidence that the presence of baby blues in the postpartum period is a significant risk factor for the development of postpartum depression, which poses a much greater danger to the mental and physical state of a woman, and also negatively affects the development of the baby. Factors in the occurrence of maternal blues include, as in the case of postpartum depression, sudden hormonal changes, as well as physical discomfort associated with various somatic disorders (ruptures, prolapse of the pelvic organs, difficulties associated with lactation). However, there are studies indicating a significant weight of psychological factors, such as the mother’s loss after the birth of a child of a sense of self-worth, which during pregnancy is often cultivated and supported by the environment. There is also evidence indicating that the incidence of postpartum sadness syndrome is associated with the emotional state of women during pregnancy. Thus, women who noted symptoms of depression during pregnancy, as well as a history of episodes of premenstrual depression, were more at risk of developing baby blues.
Thus, we can conclude that the presence of depressive symptoms during pregnancy, the occurrence of sadness syndrome in women in labor and postpartum depression are closely related and probably have common factors of formation and development.
The complexity of these factors and their heterogeneity indicates the need to take into account not only the somatic state of the woman, but also the social situation, as well as a number of psychological factors. Sources:
1. Belyaeva E. N., Wasserman L. I., Zazerskaya I. E. Postpartum depression: clinical and psychological diagnosis and assessment of the role of the psychosocial factor // Translational Medicine. – 2011. – No. 6. – pp. 29–32. 2. Harris B. Biological and hormonal aspects of postpartum depressed mood: working towards strategies for prophylaxis and treatment //The British Journal of Psychiatry. – 1994. – T. 164. – No. 3. – pp. 288–292. 3. Murray L., Cooper PJ Postpartum depression and child development //Psychological medicine. – 1997. – T. 27. – No. 2. – pp. 253–260. 4. O'Hara MW, Swain AM Rates and risk of postpartum depression—a meta-analysis //International review of psychiatry. – 1996. – T. 8. – No. 1. – pp. 37–54. 5. O'Hara MW et al. Prospective study of postpartum blues: biological and psychosocial factors //Archives of general psychiatry. – 1991. – T. 48. – No. 9. – pp. 801–806. 6. Kennerley H., Gath D. Maternity blues: I. Detection and measurement by questionnaire //The British Journal of Psychiatry. – 1989. – T. 155. – No. 3. – pp. 356–362. 7. Pitt B. Maternity blues //The British journal of psychiatry. – 1973. – T. 122. – No. 569. – pp. 431–433.
Late antenatal depression
The next three months are the time when a pregnant woman normally no longer denies her condition. In other words, her psyche has accepted the fact that there will be a child, but what she still cannot fully agree with is that with the birth of the baby, the usual way of life will come to an end. In psychology, the name of this period is quite complex. I'll voice it and then decipher it. So, this stage is called the period of “searching for a replacement for the lost object.” The lost object in this case is a familiar life, a life with a certain rhythm of work, leisure, with established relationships in the family and with friends. Gradually realizing that with the birth of a child she will have to give up a lot, the woman begins to look for a replacement for what she has lost. The classic reasoning of a pregnant woman at this stage is as follows: “Yes, I will have to leave my job, which means my career growth will stop. What a horror! But my colleagues will remain where they are, and I will be hopelessly behind them! No problem, now is the time to take a Chinese course! Relations with China are very promising, the baby will grow up, I will go to work in a new direction with a good knowledge of the language!” Thus, the second trimester becomes the most active. And indeed, the woman usually feels well, the nausea has already passed, and the stomach is not yet bothering her. And wherever expectant mothers go during this period! As they explain: “So as not to waste time.” It happens, and not rarely, that it even comes to driving courses. "Why not? The baby will be born, I will need mobility, but I still don’t have a license!”
However, this period is also ending. It is followed by the last, coinciding with the third trimester of pregnancy, which, unlike the previous one, in psychology is simply called the period of depression. That is, that same prenatal depression sets in. In the psyche there is a full awareness of what happened, and the process of saying goodbye to the past begins: “What Chinese?!” What career?! Perhaps I will never be able to work as before, but will forever be tied to pots and pans!” In the three months remaining before giving birth, at times (of course, not 24 hours a day), a woman is faced with feelings of loneliness, hopelessness and despondency. Sometimes this results in streams of tears, sometimes in irritation, resentment and anger. You can be offended and angry with your husband, whose life does not change so dramatically, and he, of course, “doesn’t understand anything and doesn’t support much.” On the mother-in-law, who always interferes with her advice and stupid purchases for the baby. For friends who are not at all interested in your belly or your child, they only care about rags, men and work. You never know what can upset a pregnant woman. All this is normal, there is no need to be afraid of your own experiences. Respect your condition and, most importantly, do not try to avoid it.
This is where we, in fact, come to the main practical conclusion. Pregnancy is not all about the joy of waiting nine months. This is the time when not very pleasant feelings and emotions are appropriate, especially in the last three months. There is no need to feel guilty, let alone shame, if in the first trimester you sometimes forgot about the baby, and sometimes even thought that it would be good if pregnancy occurred not now, but at another time.
And one more very important point. Take maternity leave on time. The fact is that the working rhythm helps a woman’s psyche stay in the first or second stage and thus not experience depression. By remaining in a familiar work environment, a woman protects herself from an acute confrontation with the awareness of drastic changes. But you can’t run away from the truth, the time will come, the baby will be born, and she will still have to understand that her old life is over forever, only this process will no longer be called pre-, but postpartum depression, and it will be harder and longer.
Although giving advice is often useless, and from the point of view of the science of psychology, it is simply unacceptable (a psychologist should help each person find their own path, draw their own individual conclusions from the current situation), I will still take the liberty of giving a few recommendations to pregnant women or already pregnant women. women who have given birth and are experiencing depression.